The development of machines that delivered a DC shock occurred in 1959 (Bernard Lown) and the first one of these devices, made by American Optical, arrived in Wellington in 1965 when I was cardiology registrar.
see left
A big advance here was that synchronised DC shocks could be delivered and thus began the application of 'Cardioversion' for elective reversion of atrial fibrillation or flutter.
An AO defibrillator was installed in the new cardiac catheter lab which opened in the Seddon Block in 1966.
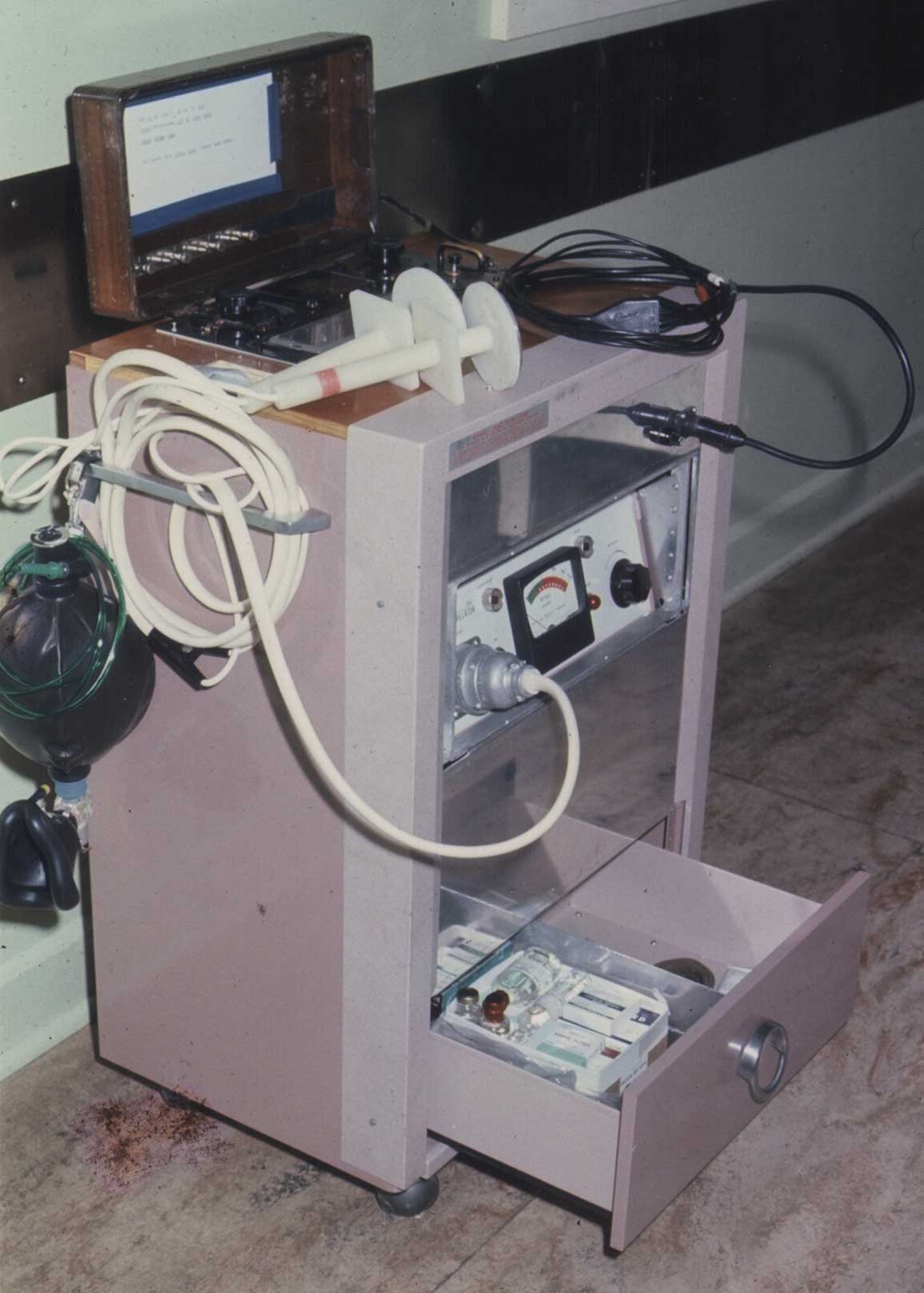
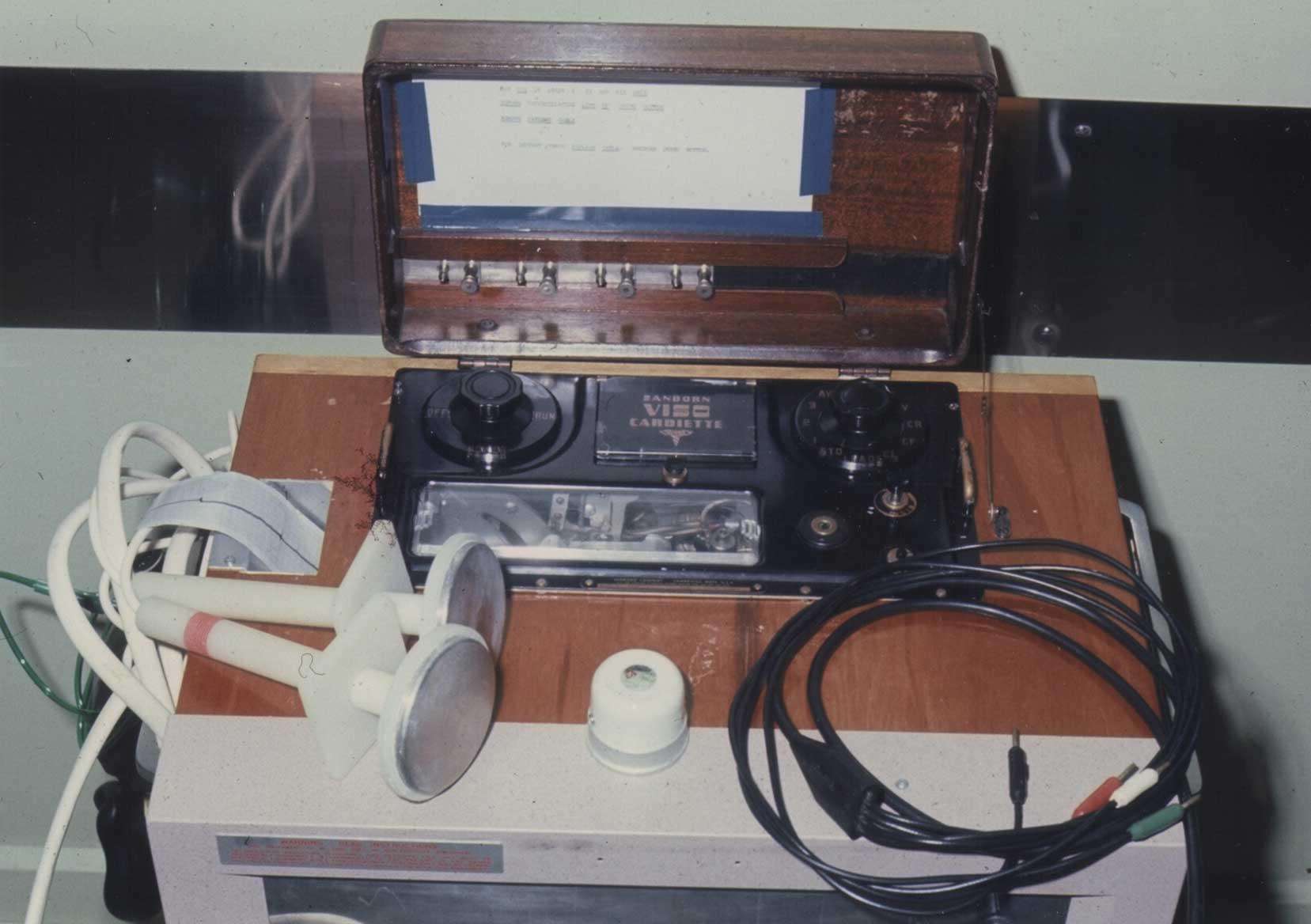
One of the early crash carts in use was a classic example of number 8 wire DIY. Don McCallum combined part of the original AO cardioverter/defibrillator along with one of the original Sanborn Viso Cardiette ECG machines in a mobile trolley equipped also with resuscitation gear.
The AO defibrillator remained in the Cath Lab until 1977 when it was replaced with one from Hewlett Packard.

A similar HP defibrillator was installed in the CCU in the Seddon Block.
In the 1980s, the CCU's HP defibrillator was replaced with the first of a series of LifePacks - initially version 3.

By the 1980s, there was placement of defibrillators at multiple locations throughout the hospital. Apart from in theatres, the cardiac catheter lab, ICU, CCU, NNU and the Emergency Department, defibrillators were also located in general ward blocks, ensuring less delay when the need arose.
For some years at least, the popular choice was the LifePack series, such as the LifePack4 seen here.


 Healthline
Healthline GP
GP Afterhours
Afterhours Hospital ED
Hospital ED